

Let's climb a mountain

Welcome to the WC.
It’s been a few weeks since I darkened your door, but we’re back in action today.
We’ve recently discussed the economics of end-of-life care a lot lately. The scam that will drain your inheritance, and a better way to allocate those funds.
Today’s a bit more personal and possibly a bit hopeful. We’re talking about cancer. What’s getting better, what’s getting worse, and what you can do today to make a small difference.
Nothing here is investment advice. Do your own research. Please.
Let’s go
Janie’s Climb

Cancer’s been on my mind a lot lately.
The disease, though calling it a single disease is a misnomer, kills millions every year. Worldwide, it’s responsible for one in six deaths.
And demographics are on its side. Due to aging global populations and bad policy choices, forecasts show that cancer will kill nearly 20 million people per year by 2050, which is a 75% increase over today.
All cancer is awful, but pancreatic cancer--with a 12% survival rate--is probably the most horrific.
Not because it’s uniquely aggressive -- though it is -- but because by the time anyone knows it’s there, it’s usually too late.
There’s no standard screening program, and it produces almost no symptoms in its early stages. You feel fine, and then one day you don’t, and then there isn’t much anyone can do.
Such was the case with Jane, my mother-in-law. 3.5 years ago, she was diagnosed with pancreatic cancer, and it took her 12 months later.
There’s not much I--an idiot with a keyboard who helps rich people make money in fun ways--can do about cancer.
But “not much” isn’t the same thing as nothing!
First
In three weeks, I’ll be lying at the base of a mountain, tucked into the fetal position, throwing up all over myself. A few hours before that, I’ll climb Puig Campana, one of the highest mountains in eastern Spain, to raise money for Cancer Care Javea.
Why?
Because three years ago, Jayne--an incredible human--spent countless hours sitting with, looking after, and being an amazing person for Jane, my mother-in-law, while she battled with pancreatic cancer.

It’s underselling Jayne’s contribution to say she made a colossal difference both to Jane and our family as we said goodbye.
Most of their funding comes from a tiny charity shop in town, and many of their materials are donated.
If you have a few (thousand??) bucks to spare, please chip in to support.
Surely my intense discomfort and possible serious injury are worth a few bucks.
Second
Let’s talk about cancer. What’s going on with the disease, the progress being made, and some realistic implications of this progress over the next several years.
Reason for hope
While cancer has demographics on its side, science is firmly in hope’s corner.
We’re finding cancer earlier.
AI-assisted imaging is now being tested across lung, breast, brain, prostate, and colorectal cancers worldwide, catching what tired human eyes miss.
A patient in China went to the hospital in early 2025 with a persistent cough. Routine chest CT looked normal. He went home.
Days later, the hospital called back -- a system reviewing his scan had flagged a shadow on his pancreas, an organ that wasn’t even the focus of the exam.
Further tests confirmed a rare pancreatic tumor. Because it was caught early, surgeons successfully removed it
“Without that alert, I would have missed my chance,” he said -- which, given a 12% survival rate, means exactly what it sounds like.
Drug discovery is compressing.
Historically, getting a new drug from discovery to approval has taken up to 15 years and cost over $2 billion, and most candidates fail in trials.
A research facility in China can now screen 300 million molecular compounds for viable drug candidates in just over a month -- the same work previously took two to three years.
In London, Isomorphic Labs -- spun out of Google DeepMind -- raised $600 million in 2025 and is preparing to put the first AI-designed cancer drugs into human trials.
The science behind it won a Nobel Prize in 2024.
Treatment is getting more personal.
As noted above, cancer isn’t a single disease. It’s hundreds, differentiated by which genes have mutated, in which cells, in which person.
Matching patients to the treatment most likely to work -- rather than the one that works on average -- is improving meaningfully. Immunotherapy response prediction for lung cancer patients is already in clinical use.
The economics of curing cancer
Better outcomes don’t just save lives. They save money. And that money can save more lives!
Cancer costs the US alone roughly 1.8% of GDP -- around $500 billion a year in direct treatment costs and productivity losses. Plus whatever economic loss comes from removing a productive 52-year-old from the workforce and family unit.

Harvard estimates that advances in diagnostics, personalized medicine, and healthcare efficiency could generate $200 to $360 billion in annual savings in US healthcare within five years -- without cutting quality or access. McKinsey puts US healthcare savings at $150 billion annually by 2030.
Those savings, thoughtfully applied, could snowball to cure Alzheimer’s disease and heart disease.
The numbers are already visible at the procedural level.
AI-assisted colonoscopy has cut procedure costs by roughly 19% in Japan and 7% in the UK. Compounded across millions of procedures a year, that’s not a rounding error.
The bigger bet is the drug pipeline. If the drugs entering human trials now -- designed in months rather than years -- perform, it restructures pharmaceutical economics from the ground up.
Shorter development cycles. Fewer failed candidates burning through capital. Faster approvals. The downstream effects on drug pricing, royalty streams, and biotech valuations are significant enough to warrant their own issue. We’ll get there.
Globally, the picture is less tidy. Cancer deaths will still rise -- ageing populations aren’t going anywhere. But the proportion that is caught early, treated correctly, and survives is shifting. That shift compounds over time, particularly in middle-income countries where the gap between specialist capacity and patient need is largest.
China is probably the best example. Enormous cancer burden, not enough oncologists, vast geographic disparity between urban and rural care.
Better diagnostics and faster drug development don’t just help patients there -- they multiply the effective workforce without training a single additional doctor.
If China’s the big winner, who are the losers?
The losers
The progress is real – it’s just not very evenly distributed.
Sub-Saharan Africa, South and Southeast Asia, and much of Latin America will likely fall behind the Global North.
Cervical cancer is the leading cause of cancer death among women in 37 countries, almost all of them in sub-Saharan Africa. It’s almost entirely preventable with an HPV vaccine, but globally, only 15% of eligible girls get the jab.
In Central and Southern Asia, it’s 1%.
That’s a policy problem science can’t fix.
For the rest, the issue runs deeper. The models driving progress in detection and drug discovery are trained predominantly on data from American and Chinese patients.
And because--I’m tapping the sign again--cancer affects different people differently, therapies that work for a soccer mom in Boston may not help a persimmon farmer in Paraguay.
One in three AI cancer diagnoses is currently vulnerable to demographic error -- misclassifying tumors in Black and Asian patients at meaningful rates because the training data doesn’t represent them.
But it’s not just technical bias.
The cancers killing the most people in low-income countries are different from the ones these models are designed to find.
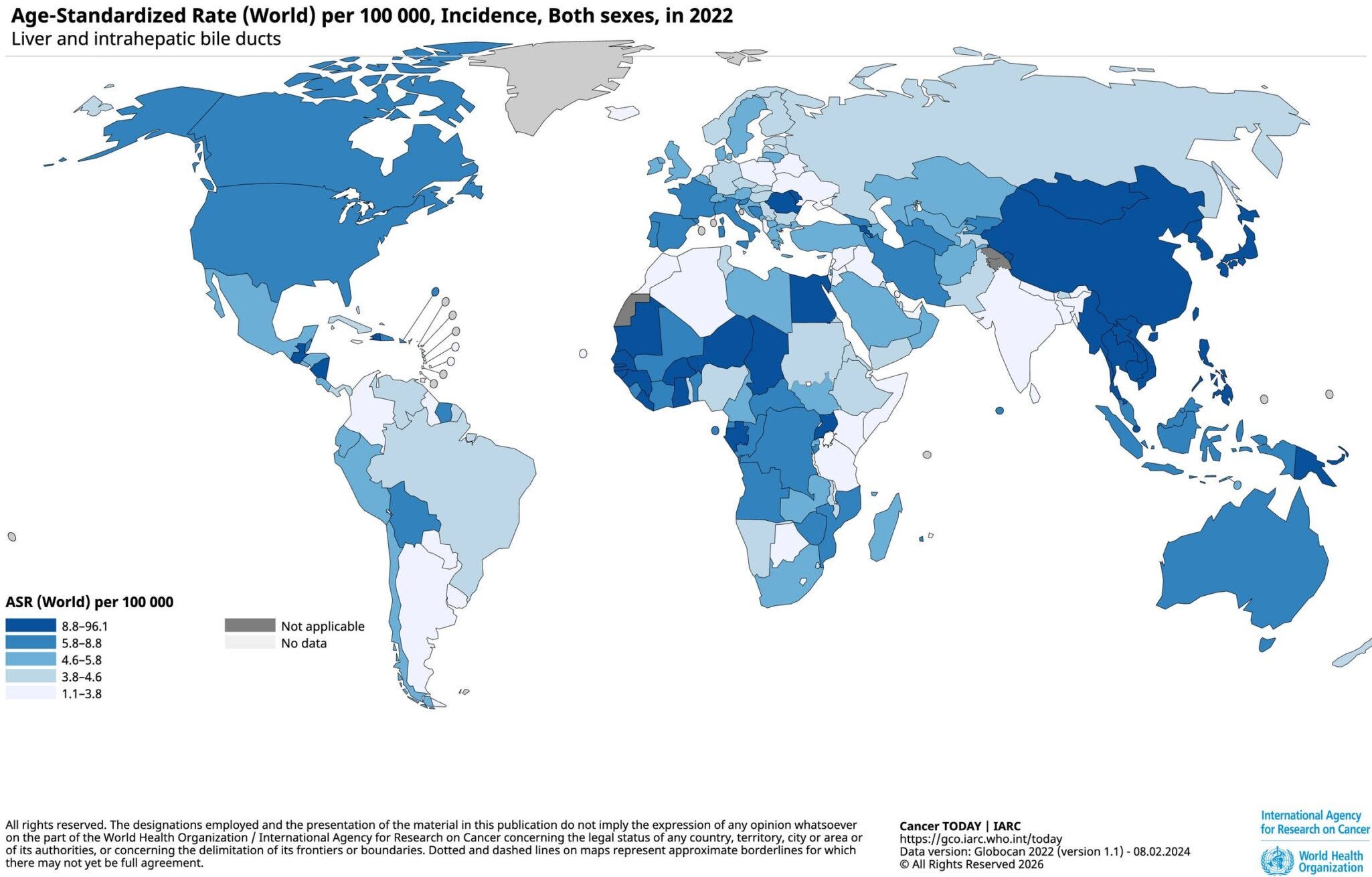
Higher rates of stomach cancer (East Asia), liver cancer (East and Southeast Asia plus sub-Saharan West Africa), and infection-driven cancers (Sub-Saharan Africa and East Asia) sythe through the developing world in ways that just doesn’t happen in wealthy Western populations.
The populations dying fastest from cancer are the least represented in the data being used to fight it.
That gap won’t close on its own. It requires deliberate, funded, international data collection -- something that’s happening, but slowly, and without the commercial incentives driving investment elsewhere.
By 2050, over half of new cancer cases and two-thirds of deaths are projected to occur in low- and middle-income countries. The tools to address that are being built. They’re just not being built for those places.
So, let’s climb a mountain
The trajectory of cancer research is, genuinely, one of the more hopeful stories in medicine right now.
Tools are improving.
Timelines are compressing.
Economics are following.
None of that helps anyone who’s sick today.
The gap between what’s coming and what exists right now is where organisations like Cancer Care Javea live.
They rely on a charity shop, donated materials, volunteers who sit with frightened people, and idiots like me climbing a mountain.
If you can spare a few bucks -- or a few thousand -- feel free to chip in.
I’ll be the one at the bottom of the mountain in three weeks. You can be the one who made it slightly worth it.
That’s all for this week; I hope you enjoyed it.
Cheers,
Wyatt
 |
|